







Introduction
Typically, organizations have some difficulty in implementing procedures in response to emergency situations, as this requires, among other things, the amount of training, drills and simulations, which can lead to an unfavorable reaction, by either the workers or the managers. In relation to the first, the direct participation in training actions is well understood and accepted, However, when it comes to train emergency and evacuation procedures, for example there are many people that do not do it easily, because it implies changes from day to day and as it is well known, the Human Being has a bit of an aversion to change to everything that is outside of the routine.
It is hoped that the situations will never occur, but in case it does, there's always the maxim that everything will be OK and what it is not well solved will be let to “destiny". It is, in fact, the acceptance in its fullfilness of Murphy's law, which says that if something has to go wrong, it will. Instead of using Prevention to prevent this maxim it is established that most people let the fatalistic spirit be installed and leave it at the care of a holy entity to determinate what happens. Such way of living can also be extensible to the management of organizations, but the main reason for which the management doesn’t encourage prevention, particularly regarding to the preparation of its elements, it is because they don’t see Prevention as an investment, which will, consequently, be a drawback to the Organization itself. Generally speaking, the cost of Non-Prevention is always higher than the cost of Prevention. Work‑related accidents, occupational illnesses and consequences of an ineffective and inefficient response to emergency situations are the most visible aspects of Non-Prevention.
If prior to the Decree-Law 220/008 of November 12th, and the Ministerial Order 1532/2008 of December 29th, respectively Legal Regime of fire safety in buildings and fire safety technical regulation on buildings, would be harder to prepare an adequate response to emergency situations, including those involving fires in buildings, by the huge disparity of standards, regulations and other documents, some of them contradictory. After the entry of these two diplomas, everything became much more simplified and easier to implement. However, there are some aspects that these two legal instruments do not cover completely, or not present with ideal clarity. The National Civil Protection Authority (ANPC) [2] issued and has been upgrading the technical notes in this context, precisely for this purpose.
Aware of this development, It has been required to the authors of projects of fire safety in buildings (SCIE) and self-protection measures (MAP) that they have adequate training, demanding and geared specifically for this purpose. Thus, the final result will have to be therefore better, with regard to this entire issue of Prevention to reduce the probability of occurrence of emergency situations, but also the protection, in order to give the best answer if prevention has not reached the desired effectiveness.
Decree-Law 220/2008 of November 12th, came typify the fairground amusements in 12 Uses-type (UT), from which we can emphasize in the framework of this study, the UT V "Hospitals and Nursing Homes". So, as for all other UT, also for this it is necessary to carry out Projects of SCIE and MAP. But, at the beginning, there is a huge obstaclet: part of the present elements in this type of facility is "bedriddenj people[…] or people limited in mobility or in reaction to an alarm" [4]. So, how can we verify the correct emergency planning? According to David Alexander, the main objective of the emergency plan is to reduce the risk of potential harmful and unforeseen [1]. The presence of people in poor mobility conditions and reduced capacity of perception and reaction to an alarm situation, makes prevention the key aspect in terms of security facilities, since the evacuation process would be strongly impaired.
In this context, it is important to properly plan all possible responses to emergency situations, to ensure that there is no need to act reactivelly. However, it’s also necessary training concrete procedures, diverse and achievable, with the aim to enable the effective and efficient response to situations that require a reactive response, i.e. after the emergency situation becomes apparent.
It is extremely difficult, if not impossible, to carry out the evacuation of some hospital facilities of medium or high dimension (with more than 1,000 staff) at once. It’s particularly important to have vaulting firewall, as it allows a quickly sectorial response, which can later be more crafted and with a greater number of means in case there is the need to expand the answer to adjacent areas, either vertically or horizontally. Thus, in hospitals, the "internal emergency plan should include special measures for self-protection, favoring the maintenance conditions of safety of occupants in the spaces, in the case of ORS, parthians and intensive care units, in case of fire, given the unpredictability of their evacuation" [4].
There is a very important figure in the context of emergency response, that is the Safety Delegate (DS). This DS is the designated person, by the person in charge of safety (RS), to direct and coordinate the measures of self-protection from the entity, in the area of fire safety and also in other situations that are likely to happen. How the DS takes the situations and the dynamism that prints to training, and drills, are fundamental for the results to be achived, since the remaining workers response will, in a long term, depend on the attitude of the DS.
Materials and Method
The case in study is a recent hospital (2012), which is part of the National Health System, but managed by a private organization. The hospital has several services (surgery, psychiatry, among others), ORS, external appointements, intermediate and intensive care day hospital and hospital admissions. The whole structure is prepared with horizontal and vertical fire vaulting. Apart from some exceptions as the main entry area, the dining hall and some storage areas, the buildings in question can fit on typology Z because "they are buildings in which each floor is split into areas that do not exceed 200 m2. In this case, the doors, have a particular fire resistance qualifications (cells)" [3].
This typology, along with the G and V, are used, for example, for determining the risk of fire, using the Gretener’s Method. On the basis of this typology of buildings present on the premises in question, and because it is guaranteed a fire partitioning horizontally and vertically, sectoral training were defined, which are intended to acquire and get better procedures for emergencies response occurring within each hospital service. However, these drills do not mingle each other because, as already mentioned, the evacuation may occur at the same flat, horizontally, and then vertically, if the emergency continues and if there is the need to give a more combined response, using the second intervention means (outside the Organization).
These sectorial training allow contiguous services to collaborate in the emergency response process. For this purpose, during training, professionals of each contiguous service are called to act, especially with first intervention means and helping in the evacuation process. This interaction causes different services of the hospital facilities to always feel supported by the employees of the contiguous services.
For each emergency situation, which can be of fire, earthquake, flood, stroke, bomb threat, or other, workers received training, based on flow charts, in that their decisions are oriented towards the resolution of the situation and, simultaneously, for his own safety and patients safety in their charge.
Once it comes to hospital facilities, we must take into account a very important aspect, which is that it is not appropriate to put patients in panic situations. Thus, in addition to train emergency response, workers have to do it quickly, but calm. If the alarm is given by horn, this may put patients and clients in a panic situation, which complicates the response process and, above all, the evacuation if necessary. The solution found and that have made very positive results is the transmission of emergency situation through a color code, where each color is associated with a situation.
For example, if there is a workout or exercise fire response in XPTO service, is heard in the sound system the message: "exercise, exercise, exercise… Red Code, XPTO service". If later is not heard any other message, is a sign that the situation was resolved. On the other hand, if then is heard the message "exercise, exercise, exercise. Green Code, XPTO service", it means that the situation is not being controlled and that it is necessary to evacuate the professionals, patients and users of the facility. In the case of a real situation, the word "exercise" is removed from the message, leaving only the remainder terms. In the formation process on the PSI given to all professionals should be given due emphasis to the explanation of the meaning of these codes, so that they are memorized by people and the response is swift and without alarm. The table below shows an example of codifying the alarm messages.
Table 1: Example of a Color Code
|
Código de Alarme |
Significado |
|
BRANCO |
Anormal situation |
|
AMARELO |
Bomb Threat |
|
CASTANHO |
Gas Leak |
|
CINZENTO |
Fuel Spill |
|
AZUL |
Earthquake |
|
VERMELHO |
Fire |
|
VERDE |
Evacuation |
Sectorial Training
Emergency planning is, above all, a process rather than a static fulfillment of objectives. Should be practiced continues and progressively and, as it is, must be adapted to the specific circumstances of the facilities and following the result of successive drills and simulations. In every workout that ran were carried out the procedures set out in the PSI, but were also made some variations or deviations from the stipulated in the same, to try to find possible loopholes for subsequent correction of the PSI and to educate workers about the fact that every emergency situation be unique, although there may be a certain type of conduct and response to resolve certain sets of same.
Training took place in some services, such as Psychiatry, Outpatient and Intensive care unit, among others. For patients of the latter, was not carried out their evacuation, as would the replacement of equipment which they are connected and of which depends on your life, and were replaced by actor people. The evacuation of the Psychiatry Service was quite satisfactory, having patients actively collaborated and follow all the indications given by the head of the queue (nurse who detected the outbreak of fire and that triggered the alarm) and the other professionals of the service and of the surveillance team, which, however, arrived on the scene and helped in the fight against sinister along with elements of a contiguous services.
The training conducted in the External consultation service, where patients were waiting for consultations, held very positively. In order to avoid being generated additional confusion caused by the presence of external elements to hospital, moments before the start of practice was warned by the technical coordinator to this patients waited for his time in the service that would be a fire-fighting training and consequent evacuation. For this purpose, were distributed by some local actor people, that as soon as they were given appointments for the evacuation, followed who performed for that purpose, having its action caused a good deal of people who waiting for consultations to join the training.
The training carried out in the area of Pediatrics brought new developments, since there is always the concern with the possible abduction of babies and children. Thus, besides the concern in response to the emergency situation created scenario, the Service had professionals whenever have the pains of the supervision of babies and children in their care. This situation is somewhat mitigated by a control system of exits and entrances of children and babies, since these have a bracelet which is placed when enter the service, and is only removed when you see given discharge. The system works by activating an alarm at the security checkpoint whenever a bracelet abandons the premises of Pediatrics. However, in emergency situations, this does not add much, particularly the emergency doors of evacuation paths, so the output of children and babies is out of control. Requires, therefore, a greater attention on the part of the profissioanis of the service, to add to what they have to pay in response to the emergency situation.
Training a lot easier, whether in the attack on the fire, either in the evacuation process was verified at the premises of the administration. The fact that the professionals working in these facilities do not have to carry out the evacuation of patients or other persons with mobility limitations, but only having to make the first intervention, and, if necessary, evacuate to the rendezvous point, meant that the practice was much more fluid. It was an important point of comparison with other services where there are not only to carry out the evacuation of the professionals, but also of users and patients, which, as already mentioned, are limited in capacity for locomotion and perception of emergency situations.
In every practice there was the collaboration of observers who noted how the various players responded to the situation by serving these notes for meetings after the training, in order to verify what was not so well, to be able to give more specific training, change the PSI, if necessary, and return the train to acquire and consolidate procedures.
As already mentioned, it is tremendously difficult to evacuate a hospital in its entirety. Thus, it is necessary to carry out evacuations resulting from sectoral emergency response processes also sectorals. In this context, the contiguous services have an important role, since the professionals of a given service where there is an emergency situation aren’t, in almost all cases, in sufficient number to give a full response to the situation, in terms of effectiveness and efficiency, taking into account that there are people with mobility limitations and perception of the alarm situation, which makes the performance of the professionals concerned.
In this context, the widespread alarm message by sound system is given not only to the service where the emergency situation takes place, but also the contiguous services. The professionals of these services, when hearing the message, know they have to travel to the affected Service, in order to assist in the emergency response process, in particular in fighting fire with means of first intervention and in the process of evacuation of patients and users.
The evacuation of a particular service should be made horizontally, to the contiguous floors and then, depending on the seriousness of the situation and the condition of the patients, give up early, with more time, a complementary evacuation procedure for the lower floors or rendezvous points outside the premises, depends on the case. Fire compartmentalisation assumes a prominent role here, because it ensures a very important time for professionals to stabilize patients recovered quickly and the service forward, if necessary, to other locations.
In installations where there is no fire vaulting this evacuation process becomes more complicated, since patients can’t be evacuated to contiguous services and remain there; on the contrary, must be evacuated to lower floors or to the exterior of the building, which complicates the process. It is therefore important that the vaulting fire work, namely the doors. Some of these are open and stuck to the walls with electromagnets. So it is given a code red, the doors should close automatically, fulfilling its function of fire compartmentation.
Should not, therefore, be arrested or held open by another process that not only the electroínames. In some situations, people, by ignorance of the fire compartmentation function, keep the doors open with wedges between the floor and the doors. This practice is extremely dangerous, because the doors will not close and thus holding the fire a given space will not check. There is also mention that, in this situation, the smoke-clearing system also is not effective, since the volume of air to take off feeding is quite superior. As it comes to hospital facilities, in which we must move some patients on stretchers and beds, if the doors are closed in a situation of normality, very difficult this same movement of patients. The solution is by placing electromagnets attached to the doors of vaulting.
There is another situation that has to be taken into account, which is the opening emergency doors only in the sense of the evacuation. If this assumption is a measure that prevents the return to the location of the emergency, is an impediment to the professionals of contiguous services, since it does not allow them access to facilities emergency target. They just can get it when there's someone coming in the direction of evacuation, or when the surveillance personnel, which has control over all ports, accompanies them. Therefore, it is necessary the training and practice of these actions, for the precious help of contiguous services professionals arrive in a timely manner to the affected Service.
In PSI are provided some actions-type to be performed in emergency situation. As the emergency situation on the fire is the most common, it is the most trained and which has greater expression in the document. The following flowchart (Figure 1) illustrates the actions to be taken and those involved in the overall process of response to a fire situation.
Training versus Drills
During general training given to all hospital workers, including those who provide occasional service premises above the minimum days laid down in legislation (more than 30 days per year), it was explained the fundamental difference between a workout and a simulacrum: a workout, people know that the exercise will be held at a certain day and hour, are educated and trained on the procedures to be implemented in the event of an emergency and repeated the number of times necessary until it acquired the proficiency needed for the effectiveness and efficiency of the response are desirable.
On the other hand, a simulacrum worthy of this name, the workers do not know the day nor the hour in which they will have to respond to the emergency situation ... just know it will within a broad timeline set in a timely manner. There are, however, some key people who have, necessarily, to have knowledge of the accomplishment of simulacrum, which are essentially: the person in charge of safety, the DS, the PSP or GNR Commander, Commander of the Firefighters, the ANPC (local) and one or another person whose functions in hospital facilities are of limited importance for the response to the emergency.
The main objective of a drill is to test the response, in time, effectiveness and efficiency. When preparing a scenario for a simulacrum and warn all stakeholders that the same will happen, specifying the time and place, you're not exactly perform a drill, but a workout, since people are already alert to the situation. A drill is an approximation as possible to a real situation. The real situations of emergency don't warn previously: just happen! Thus, if stakeholders are advised, theyr ability to truly answer is not tested, so it is important to define when it comes to a workout or exercise and a drill.
No tests truly none of these aspects if workers learn that will take place a simulacrum in determined day and time because it will prepare everything very close to this timeline so that your answer is the best. Simply is not tested anything with this type of event (mixed with exercise and drill), only to lose time, because they don’t chek their acts truly, nor procedures to test the responsiveness of the more about possible reality. And the reality brings emergency situations that do not warn ... It is therefore appropriate that all are more adverse scenarios devised, so that the training is for the worst possible situations. A scenario can be defined as a model of conditions and circumstances and is usually created to illustrate how the conditions influence the circumstances and how these change those (Alexander, 2009).
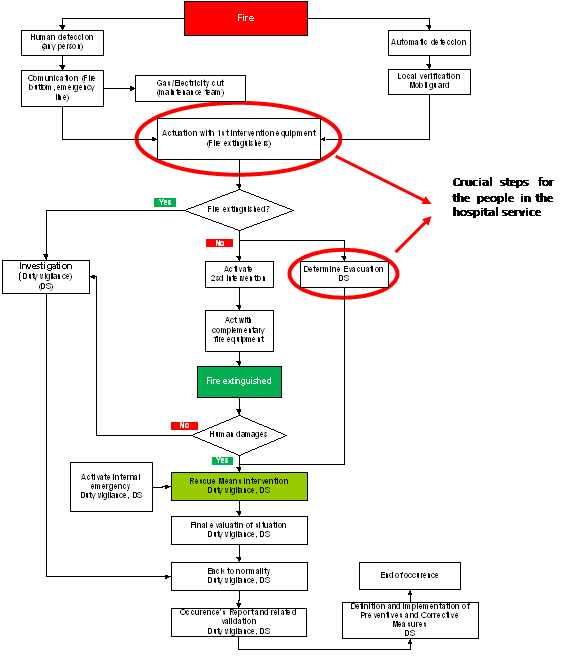 |
Figure 1- Fire Flowchart Procedures
Results and Discussion
Along the training being conducted in three-hour blocks for sets of 20 elements, on average, in general terms, it was reported that the materials had been understood and that the procedures in the event of an emergency would be assimilated. However, throughout the first sectoral training in some of the services of the hospital unit, one of the commonalities reported by observers of the exercises was that a significant proportion of those involved in combating the sinister and in the evacuation of patients showed some confusion, if not even apparent ignorance of procedure. This observation gave rise to a more incisive action, in terms of training.
On the other hand, even with this apparent uneasiness in response, the average times for the evacuation of various services were around 15 minutes. If one consider the fact that this hospital has fire vaulting, the sinister fighting time and consequent evacuation of service cannot be considered high, because it involves the movement of patients with physical and psychological limitations, some of which are in extremely serious situations.
It should be noted that, in the places that receive public, as in the case of hospital units, drills are carried out in response to emergency situations. The achievement of these trainings prepare not only the professionals, as well clients and patients who are more aware of reality and with greater mobility. The acquisition of routines by all causes the appropriate response in emergency situations is more natural and don't make both a timeline of decision‑making about what to do in that context.
The presence of strange people at the premises, in particular the patient relatives or visitors can be a serious obstacle to an evacuation procedure, because these people can react in a panic attitude, which is unadvisable. Some may even want to pick up the sick relatives, which can jeopardize your life, of families, of profissioanis and seriously complicate the process deposed to the emergency. Thus, the proper preparation of the professionals of the facilities is crucial, because it will make their action be calm and incisive, allowing control of any situations of panic on the part of relatives and other visitors and even patients.
Another situation that must be taken into account and explore from the point of view of lessons learned, is conducting debriefing meetings after training and Simulacrum. These meetings must be between key players, since they are the range of good practice, so that they are repeated, but are also covered aspects that went less well or not go at all well.
Participants should not face the debate about these negative aspects as a pointing finger, a form of criminality or of accountability for actions less successful. On the contrary, must face these meetings in order to remove these teachings to train what went less well and get in future workouts or simulacrum, give an answer to not fail again in the errors pointed out. It is therefore important to understand this objective on the part of who participates in training or simulacrum. It is also important that the practice or of Simulacrum Coordinator point the flaws, the procedures themselves, and never the people who failed, since what is at issue is the incorrect procedure, which may have been committed by the person A or B, no matter. It matter, yes, we all know that doing things in a particular way didn't work and that, therefore, the correct or improve.
Conclusions
The response to emergency situations in hospital units of any dimension is not an easy process, if it is viewed in a global way, i.e. to engage the entire hospital unit. Therefore, it is important to carry out the sectoral training, according to the fire compartmentation which exists on the drive in question. In this way, one can not only take advantage of the elements of each service, as well as contiguous services elements, is it being given the general alarm for the entire unit, contiguous services professionals to what is emergency target can collaborate in response to this, allowing for greater effectiveness and efficiency in the process. The workouts carried out at the moment allowed come to this realization.
Regardless of the theoretical knowledge that professionals of the hospital units may have in relation to procedures that they must execute when subjected to emergency situations, it is with some trepidation that it appears that, in practice, and due to the fact of having to be evacuated and the evacuation of patients in their care, such procedures are not carried out with the quickness.
Thus, it is extremely important to perform periodic workouts to ensure that the procedures are internalised and do not oblige both a phase of thinking about what actions to take, namely, that they become natural. The drill required legally will then test the quality of the response and demonstrate if the practice was enough and the objectives achieved.
Acknowledgments
A preliminary version of this paper has been presented at ORPconference 2014.
References
- 1. Alexander, D. (2009). Principles of Emergency Planning and Management. (5th ed.). MGP Book Group.
- 2. ANPC (2009). Segurança Contra Incêndio em Edifícios (1ª ed.). Lisboa: Europress.
- 3. Leça Coelho, A. (2010). Incêndios em Edifícios (1ª ed.). Alfragide. Edições Orion.
- 4. Miguel, M., Silvano, P. (2010). Regulamento de Segurança em Tabelas. (2ª ed.). Fábrica das Letras.
Papers relacionados











